Retinal Birefringence Scanning
 Our laboratory has been
developing novel technology for detecting accurate eye alignment directly, by
exploiting the birefringence (property that changes the polarization of light) of
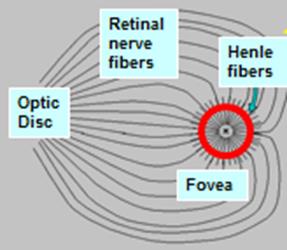
the uniquely arranged nerve fibers (Henle fibers) surrounding the fovea (the
small area of the retina, responsible for sharp central vision). Retinal
birefringence scanning (RBS) is a technique that uses the changes in the
polarization of light returning from the eye to detect the projection into
space of the array of Henle fibers surrounding the fovea. In RBS, polarized
near-infrared light is directed onto the retina in a circular scan, with a
fixation point in the center, and the polarization-related changes in light
retro-reflected from the ocular fundus are analyzed by means of differential
polarization detection. Due to the radially symmetric arrangement of the birefringent Henle fibers, a characteristic frequency
appears in the obtained periodic signal when the scan is centered on the fovea,
indicating central fixation. By analyzing frequencies in the RBS signal from
each eye, the goodness of eye alignment, and thus strabismus, can be measured.
In preliminary studies and in an early prototype, RBS has demonstrated reliable
and non-invasive detection of foveal fixation, as
well as detection of eye misalignment.
Our laboratory has been
developing novel technology for detecting accurate eye alignment directly, by
exploiting the birefringence (property that changes the polarization of light) of
the uniquely arranged nerve fibers (Henle fibers) surrounding the fovea (the
small area of the retina, responsible for sharp central vision). Retinal
birefringence scanning (RBS) is a technique that uses the changes in the
polarization of light returning from the eye to detect the projection into
space of the array of Henle fibers surrounding the fovea. In RBS, polarized
near-infrared light is directed onto the retina in a circular scan, with a
fixation point in the center, and the polarization-related changes in light
retro-reflected from the ocular fundus are analyzed by means of differential
polarization detection. Due to the radially symmetric arrangement of the birefringent Henle fibers, a characteristic frequency
appears in the obtained periodic signal when the scan is centered on the fovea,
indicating central fixation. By analyzing frequencies in the RBS signal from
each eye, the goodness of eye alignment, and thus strabismus, can be measured.
In preliminary studies and in an early prototype, RBS has demonstrated reliable
and non-invasive detection of foveal fixation, as
well as detection of eye misalignment.
Retinal birefringence
scanning is innovative technology developed by two colleagues (Drs.
David Guyton and David Hunter) in the Johns Hopkins Department of
Ophthalmology. When I joined the department in 2000, I added to their expertise
my experience – in electronics, optoelectronics, signal processing, computer
programming, and modeling – to design and build the first prototype of a vision
screener that employs retinal birefringence scanning for strabismus detection.
Clinical testing of that device validated the principle of operation and showed
remarkable performance in some patients. But technical limitations that caused
relatively high optical noise (contamination of the signal with unwanted light)
in the instrument, as well as significant variation of the signal level among
individuals, thwarted its commercial development, and the device did not reach
clinical application. We now propose to build on the lessons learned from that
early work, which involved studying the physiological phenomenon, making
quantitative assessments, studying the opportunities, and developing basic
technologies.
The principle of RBS is
explained in more detail in the following illustrations:
|
|
|
The fovea is the most
sensitive part of the retina. The object of fixation is projected onto it. |
With proper central
fixation, the point of fixation should be projected in the center of the vovea.
|
|
|
Detecting central
fixation is done by checking the location of the fovea |
The location of the fovea
can be detected by scanning around its presumed center.
|
|
|
|
When illuminated with
polarized light (such as the light coming from a low-power laser), the Henle
fibers surrounding the fovea change the polarization state of light and
create a bow-tie pattern. |
|
|
|
|
The simplest and
fastest way to check whether the eye is fixating properly is to use circular
scanning around the expected center of the fovea. |
Here is exactly how it
works:
|
|
|
The basic principle
of RBS Device functioning is based on detecting the location of the
polarization cross which cross coming from the retinal nerve fibers which
exhibit optical birefringence, especially the radial array of Henle fibers,
containing neurotubules whose diameter is
comparable to the wavelength of the near-infrared light. Birefringence is a
property of materials to change the polarization state of light. So, we need
a simple and fast method to tell us whether the fovea is where it should be
during central fixation. With the eye fixating properly (central fixation), the fovea is
encircled by the scanned annulus. The concentric circle of light falls
entirely on the radial array of Henle fibers and generates a signal which is
twice the scanning frequency. With other words, we have doubling of the
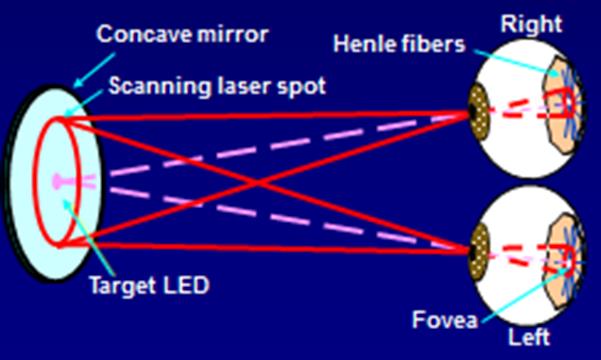
scanning frequency, if the fovea is where it should be. By arranging for both eyes to view the same target, and by separately
detecting the signals emerging from the two eyes, we can detect proper
fixation by both eyes simultaneously, and thus detect proper alignment of the
two eyes. |

The basic principle of
RBS is illustrated in the figure above. More precisely, due to the strict
radial symmetry of the Henle fibers about the fovea, retinal birefringence
causes the polarization state of linearly polarized light to change at “whole
multiples” of the frequency of the circular scan, such as at twice the scanning
frequency as described in detail previously.
While automated
screening tools exist, very few are effective in truly detecting where the eyes
are looking. The novel technology we are developing will tell when both eyes
are looking in the desired direction by detecting the actual fovea of each eye
– the part of the retina that we aim at objects when we look at them. With a
hand-held instrument from 12 inches away, we scan the retina with a spot of
polarized near-infrared light in a circle, a technique we call “retinal
birefringence scanning” (RBS). Our Pediatric Vision Screener will combine a new
version of RBS for detecting strabismus accurately, with added technology for
assessing proper focus of both eyes simultaneously, and optimized electronics
and signal processing to ensure high-quality signals. By enabling early
identification and treatment of children at risk for amblyopia, this instrument
has the potential to prevent lifelong disability from a readily treatable
condition.
|
|
|
The simplest method to detect the central and
para-central frequencies is to use the Fast Fourier Transform. |
Alignment detection
For each eye, if the scanned circle of polarized
near-infrared light is centered on the fovea, the signal of the returning light
has a strong frequency component that is a specific “multiple of half”
frequency of the scan frequency, determined by the fractional frequency of the
HWP, indicating central fixation. Spectral analysis by means of the Fast
Fourier Transform (FFT) for each eye reveals whether a subject is fixating on
the target with one eye, both eyes, or neither eye.
Binocular
fixation and alignment detection
We also need to assess proper fixation of both eyes simultaneously:
|
|
|
The position of the fovea is checked simultaneously
for both eyes, both fixating on the same target. |
In
the 2002 prototype of the pediatric vision screener this is accomplished via
the following binocular design:
More on Retinal
Birefringence Scanning, including improved technologies:
1. Gramatikov, BI, Irsch, K, and Guyton, D; "Optimal timing of retinal scanning during dark adaptation, in the presence of fixation on a target: the role of pupil size dynamics. Journal of Biomedical Optics, 2014, 19(10), 106014. doi:10.1117/1.JBO.19.10.106014.
http://biomedicaloptics.spiedigitallibrary.org/article.aspx?articleid=1921066%20&journalid=93
2.
Irsch,K., Gramatikov,B.I., Wu, Y. K., Guyton,D.
L. A new pediatric vision screener
employing polarization-modulated, retinal-birefringence-scanning-based
strabismus detection and bull’s eye focus detection with an improved target
system: Opto-mechanical design and operation. Journal
of Biomedical Optics, 2014, Jun 1;19(6):67004. doi:
10.1117/1.JBO.19.6.067004.
http://biomedicaloptics.spiedigitallibrary.org/article.aspx?articleid=1881172
3.
Gramatikov,
B. Modern Technologies for retinal
Scanning and Imaging. An Introduction for the biomedical Engineer.” An invited review, Biomedical Engineering OnLine, 2014, 13:52; DOI:
10.1186/1475-925X-13-52. Published April 29, 2014.
http://www.biomedical-engineering-online.com/content/13/1/52
- Irsch, K, Gramatikov, B.I.,
Wu, Y-K, Guyton, D.L. Improved eye-fixation detection using
polarization-modulated retinal birefringence scanning, immune to corneal
birefringence. Optics Express, 22(7):7972-7988, published on 18 March
2014, DOI:10.1364/OE.22.007972, http://www.opticsinfobase.org/oe/abstract.cfm?uri=oe-22-7-7972
http://www.opticsinfobase.org/oe/fulltext.cfm?uri=oe-22-7-7972&id=282349
5.
Gramatikov, B. Detecting fixation on a target
using time-frequency distributions of a retinal birefringence scanning signal. BioMedical Engineering OnLine 2013, 12:4. Published on May
13, 2013. doi:10.1186/1475-925X-12-41
http://www.biomedical-engineering-online.com/content/12/1/41.
6.
Gramatikov,B., Irsch,K., Müllenbroich,M., Frindt,N., Qu,Y., Gutmark,R. Wu,Y.-K.,
Guyton, D. A Device for Continuous Monitoring of True Central Fixation Based on Foveal Birefringence. Annals of Biomedical Engineering, Vol.
41, Issue 9 (1 Sept 2013), pp. 1968-1978.
Also Epub ahead of print: May 4, 2013. DOI: 10.1007/s10439-013-0818-2. PMID: 23645511.
http://link.springer.com/article/10.1007%2Fs10439-013-0818-2
7. Irsch,
K., Gramatikov, B., Wu, Y.-K., Guyton, D.
Modeling and
minimizing interference from corneal birefringence in retinal birefringence
scanning for foveal fixation detection. Biomed
Opt Express. 2011 Jul 1;2(7):1955-68.
http://www.opticsinfobase.org/boe; http://www.ncbi.nlm.nih.gov/pubmed/21750772
8. Agopov M., Gramatikov B.I., Wu Y.K., Irsch K, Guyton
D.L. Use of retinal nerve fiber layer
birefringence as an addition to absorption in retinal scanning for biometric
purposes. Applied Optics, 2008, Mar 10; 47 (8):1048-53,
http://www.ncbi.nlm.nih.gov/pubmed/18327275
https://www.osapublishing.org/ao/abstract.cfm?URI=ao-47-8-1048
9.
Gramatikov B.I., Zalloum
O.H.Y., Wu Y.K., Hunter D.G., Guyton D.L. A Directional Eye Fixation Sensor Using
Birefringence-Based Foveal Detection. Applied Optics, Vol. 46, Issue 10, pp.
1809-1818, April 2007,
https://www.osapublishing.org/vjbo/fulltext.cfm?uri=ao-46-10-1809&id=130944
10. Gramatikov B.I., Zalloum
O.H.Y., Wu Y.K., Hunter D.G., Guyton D.L. Birefringence-based eye fixation monitor with no moving
parts. Journal of Biomedical Optics, 2006, 11(3), May-June, pp. 034025-1 -
034025-11,
http://www.ncbi.nlm.nih.gov/pubmed/16822074
http://www.sciencedirect.com/science/article/pii/S0886335004009484
- Hunter D.G., Nassif D.S., Piskun N.V.,
Winsor R., Gramatikov B.I., Guyton D.L.
Pediatric Vision Screener 1: instrument design and operation. Journal of Biomedical Optics,
2004 Nov;9(6):1363-1368.
http://biomedicaloptics.spiedigitallibrary.org/article.aspx?articleid=1101874
- Nassif D.S., Piskun N.V., Gramatikov B.I., Guyton D.L., Hunter
D.G. Pediatric Vision Screener 2:
pilot study in adults. Journal
of Biomedical Optics, 2004 Nov;9(6):1369-1374,
http://www.ncbi.nlm.nih.gov/pubmed/15568960